
‘Anyone can get an infection and almost any infection can lead to sepsis, the body’s extreme response to an infection.’¹ If not or improperly treated, this can rapidly lead to tissue damage, organ failure, and/or death.
This is the opening statement of one of the latest Centers for Disease Control and Prevention (CDC) fact sheets on antibiotic-resistant infections.
Surgical site infections (SSIs) represent one of the most frequently reported types of hospital-acquired infections (HAIs), constituting up to 19.6% of all HAIs in Europe in 2011 and 2012.² Depending on the type of surgery, SSIs cause a significant burden—both economically and in terms of a loss of years with full health.³
Economical impact of SSIs
The increased length of stay is responsible for the majority of additional healthcare costs,⁴ ⁵ followed by parenteral medication (administered or occurring elsewhere in the body other than the mouth and alimentary canal) and additional surgical procedures.⁶ ⁷
To put this into perspective, a recent Dutch study (M.B.G. Koek et al, 2019) has measured the economic impact of treating SSIs in three of the most commonly performed types of surgery: colectomy, mastectomy and total hip arthroplasty (THA). The results were unsettling. The attributable costs per SSI were €21,569 (THA), €14,084 (colectomy) and €1,881 (mastectomy). If projected nationally, these costs would equal to €10 million, €29 million and €0.6 million, respectively. Although these estimations have been calculated based on the healthcare costs in the Netherlands, it is reasonable to assume the cost will likely be very similar for many other European countries.
Sources of infections
The operating theatre is historically one of the departments where infection control has been more challenging due to a number of reasons, including:
- The constant flow of patients going in and out of the theatre
- OR Staff carrying out a wide range of procedures
- Continuous exposure to pathogens (blood, body fluids and tissues).
In a controlled environment, one might question what factors could cause or contribute to the development of infections. Ordinarily, infections originate by pathogens being present in the operating theatre environment.
Blood-borne pathogens
These pathogens include hepatitis B (HBV), hepatitis C (HCV) and human immunodeficiency virus (HIV), and they are transmittable when blood or body fluids from an infected person enter another person's body via injections, cuts, abrasions.
Bacteria present on operating theatre surfaces
These include the inanimate environment in operating theatres (e.g. tables, floors, and equipment surfaces).
Such bacteria are considered potential vectors of pathogens that may cause SSIs. Although most of these are treatable with antibiotics, some of them have built a resistance to several drugs. Arguably, the most recognised of these bacteria is the methicillin-resistant staphylococcus aureus (MRSA), an antibiotic-resistant bacteria responsible for several infections that are difficult to treat in humans and are quite common in hospitals’ settings.
Micro bodies (such as lint)
It is important to emphasise that micro bodies (including cornstarch powder⁸ and fibres⁹ ¹⁰ ¹¹) may carry microorganisms and these can be deposited directly or indirectly into surgical wounds and generate infections. The fabrics from which items used in the operating theatre are made of vary tremendously in their capacity to generate lint.¹² For example, washed cotton fabrics are more easily eroded compared to polypropylene. The main reason is that the polypropylene (SMS) microstructure is made of continuous filaments welded together at frequent points to prevent accessibility to the strands. This characteristic structure makes it difficult to create lint.

Figure 1
280–count Polyester/Cotton washed
The photomicrograph illustrates the most commonly used surgical fabrics materials. These materials will likely produce lint when the material rubs against itself, the surgical table or other objects.¹³
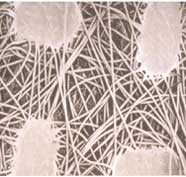
Figure 2
Polypropylene SMS (Spunbond/meltblown/spunbond)
Polypropylene is a much smoother material with weld points to anchor the extremely long polypropylene filaments. This makes it more difficult to create lint.¹³
The Importance of appropriate infection prevention and control measures
In order to reduce the risk of surgical site infections, the risk of microbial contamination of the surgical site from the theatre environment needs to be minimised. Below are some of the key actions that could potentially help with preventing and/or limiting these costly post-operative complications.
Blood-borne pathogens
One of the ways to neutralise the risk of the transmission of blood-borne pathogens is effective sterilisation of surgical instruments. That is in addition to the effective containment and disposal of all the other devices that are in contact with a patient’s body (that could potentially expose them to infections).
Bacteria present on operating theatre surfaces
Handling multiple patients during varying procedures in a single day requires consistent processes and practices to ensure that each patient is in the safest environment possible. Having consistent cleaning practices in place between surgeries could also help with reducing the risk of cross-contamination.
Micro bodies
While it is nearly impossible to reduce all of the lint that is shed, it is possible to significantly reduce it. One strategy amongst the many for infection prevention and control could be the selection of low-lint or lint-free products, which in turn could lessen the risk of infections.
Visit our operating theatre table products to help prevent or manage SSIs.

Anna Marogna
Product Manager, Medline Europe
Anna, a native of Italy, holds a BSc. in International Trade (Verona) and an MSc. in International Marketing (London, UK)—the foundation of her over 3 years of experience in the international healthcare industry. She is a lover of green spaces and the general outdoors, and currently manages Medline’s operating table covers and primary care portfolios at the European level.
Reference:
1. https://www.cdc.gov/drugresistance/pdf/threats-report/Threat-Modern-Medicine-508.pdf
2. European Centre for Disease Prevention and Control, Point prevalence survey of healthcare associated infections and antimicrobial use in European acute care hospitals (2011–2012). Available at: http://ecdc.europa.eu/en/publications/Publications/healthcare-associated-infections-antimicrobial-use-PPS.pdf
3. Cassini A, Plachouras D, Eckmanns T, Abu Sin M, Blank HP, Ducomble T, et al. Burden of six healthcare-associated infections on European population health: estimating incidence-based disability-adjusted life years through a population prevalence-based modelling study. PLoS Med 2016;13:e1002150
4. Tanner J, Khan D, Aplin C, Ball J, Thomas M, Bankart J. Post discharge surveillance to identify colorectal surgical site infection rates and related costs. J Hosp Infect 2009;72:243-50.
5. MongeJodra V, Sainz de Los Terreros Soler L,Diaz-Agero Perez C, Saa Requejo CM, Plana Farras N. Excess length of stay attributable to surgical site infection following hip replacement: a nested case e control study. Infect Control Hosp Epidemiol 2006;27:1299-303.
6. Edwards C, Counsell A, Boulton C, Moran CG. Early infection after hip fracture surgery: risk factors, costs and outcome. J Bone Joint Surg Br 2008;90:770-7.
7. Kashimura N, Kusachi S, Konishi T, Shimizu J, Kusunoki M, Oka M, et al. Impact of surgical site infection after colorectal surgery on hospital stay and medical expenditure in Japan. Surg Today 2012;42:639-45.
8. Newsom SWB, Shaw P. Ariborne particles from latex gloves in the hospital environment. Eur J Surg 1997: 163 (Suppl 579):31-3.
9. Edmiston C, Sinkski S, Seabrook G, et alt. Airborne particulates in the OR environment AORN J 1999;69(6): 1169-83.
10. Glasgow D, Sommers J. Lint shedding cannot be overlook. Clin Serv J 2003: 28-30.
11. Verkkala K, Eklund A, Ojajarvi J, et alt. The conventionally ventilated operating theatre and air contamination control during cardiac surgery-bacteriological and particulate matter control garment options for low level contamination. Eur J Cardiothorac Surg 1998: 14(2): 206-10.
12. Edmiston C, Sinkski S, Seabrook G, et alt. Airborne particulates in the OR environment AORN J 1999;69(6): 1169-83.
13. Truscott W. Impact of microscopic foreign debris on post-surgical complications. Surg Technol Int. 2004;12:34-46. PMID: 15455309

